Laser Spine Institute Patient Authorization for Release of Medical Information 2014-2024 free printable template
Show details
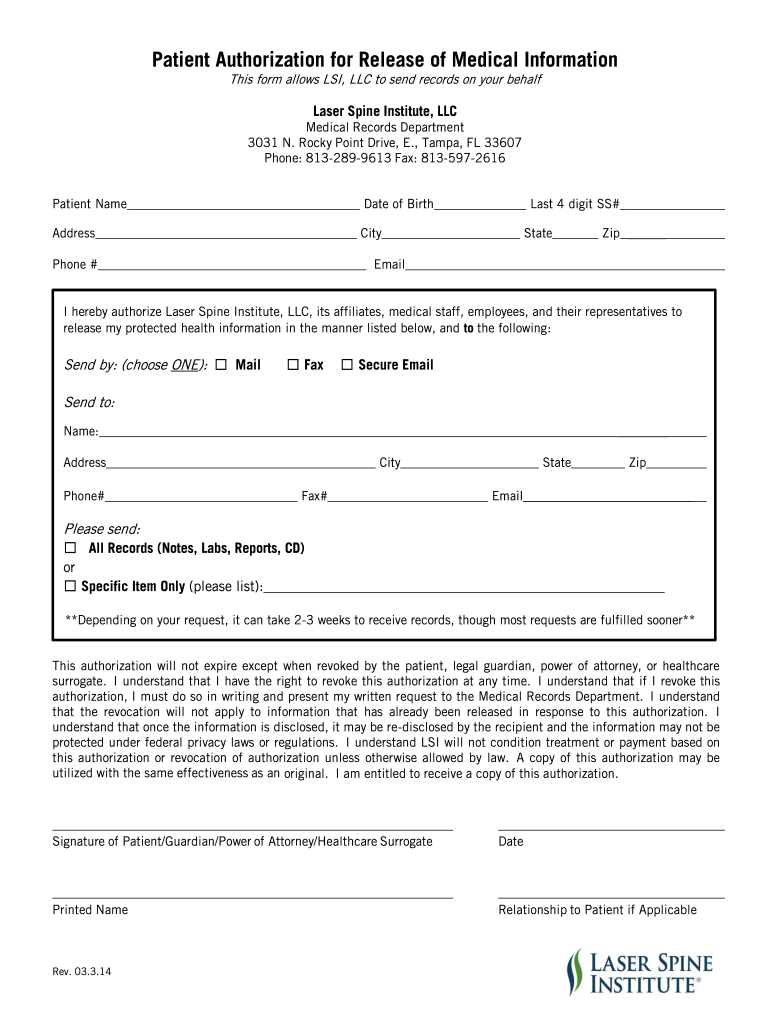
Patient Authorization for Release of Medical Information This form allows LSI LLC to send records on your behalf Laser Spine Institute LLC Medical Records Department 3031 N. Rocky Point Drive E. Tampa FL 33607 Phone 813-289-9613 Fax 813-597-2616 Patient Name Date of Birth Address City Phone Last 4 digit SS State Zip Email I hereby authorize Laser Spine Institute LLC its affiliates medical staff employees and their representatives to release my protected health information in the manner listed...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign
Edit your medical records release form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your medical records release form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing medical records release form online



To use our professional PDF editor, follow these steps:
1
Log in to your account. Start Free Trial and register a profile if you don't have one.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit hipaa medical records release form. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
How to fill out medical records release form
How to fill out a medical records release form:
01
Begin by obtaining a copy of the medical records release form from the healthcare provider or facility where your records are held.
02
Carefully read through the form to ensure that you understand all the information required and any specific instructions provided.
03
Fill in your personal information accurately, including your full name, date of birth, address, and contact details.
04
Provide the name and contact information of the healthcare provider or organization that you authorize to release your medical records.
05
Specify the purpose for which the medical records are being released, such as for personal records, legal proceedings, or for a new healthcare provider.
06
Indicate the timeframe for which the medical records release is valid, if applicable.
07
Sign and date the form, acknowledging your consent for the release of your medical records.
08
If required, have any additional parties involved, such as a legal guardian or power of attorney, sign the form as well.
09
Make copies of the completed form for your records and submit the original to the healthcare provider or facility.
Who needs a medical records release form:
01
Individuals who wish to transfer their medical records from one healthcare provider to another may need a medical records release form.
02
Patients who are enrolling in a new healthcare facility or starting treatment with a new healthcare provider may be required to complete a medical records release form.
03
In legal matters, attorneys may require their clients to sign a medical records release form to access relevant medical records for a case.
04
Insurance companies or government agencies may also require a medical records release form to verify or process claims.
05
Family members or individuals acting on behalf of a patient may need to submit a medical records release form in order to access their medical information.
Note: Specific requirements regarding the need for a medical records release form may vary depending on the jurisdiction and policies of the healthcare provider or organization involved.
Video instructions and help with filling out and completing medical records release form
Instructions and Help about physician form record
Hello Dave Guerra real record service how are you thanking you for stopping by today to watch this video today I'm going to talk about the authorization to release health information form it's usually a one-page document I know another medical document you have to fill out, but you know what this is for your own protection because again this lets the hospital the private practice or the clinic know what you need why you need it and who accessed it and who gave it to you the whole nine yards which is a good thing especially when your privacy is at stake, so ideally I'm going to go over the farm from top to bottom and what I'm looking at or what you're going to see is you show up at the medical records department at the clinic or the doctor's office you say hey I need a copy of my medical records well they're going to hand you a form typically like I said one page now they might go into — it just depends on your location there might be your state might require additional notifications that's okay that's strictly up to them so but for the most parts I've encountered one-page documents and usually cram everything in there, but please read the entire document before you fill it out again read the entire document before you start putting your name on that piece of paper now at the top of the form should say the practice the hospital or the clinic that's it has the information next there should be a title and bold letters will say authorization and disclose protected health information authorization to disclose medical records authorization to release protective wealth wise percent protected or health information or medical information again then the next section would be your name we're not necessarily your name the patient's name and that would be like the legal representative you would be the legal representative you would need to put the patient's name down there we go sorry about that, and then you put the patient's full name not like Jake you actually put Jacob not Tony unless that's what it is in his birth certificate NATO how they signed in you would put Anthony otherwise the date of birth now you may be asked for additional information that's okay because again how many Jon semesters in the world and how many John Smith's share the same birthday so again now you might be asked like I said for additional information this would typically be like your address or your social security number maybe like the last four digits or if you have a medical record number that's okay if you don't know problem between you and the medical record clerk you guys you will definitely drill down to get exactly your information the next section will be where you or the legal representative of the patient will authorize the facility the hospital the clinic the private practice and will be written on there or in some cases you have to fill it out yourself that's okay, and you authorize them to disclose the information relating to the above-named individuals' health...
Fill physician form copy : Try Risk Free
People Also Ask about medical records release form
How do I get my medical records from a retired doctor in BC?
Can I get my medical records from my doctor in BC?
What is Form 14 release of information Ontario?
How do I get my medical records in Quebec?
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is medical records release form?
A medical records release form is a document used to authorize the release of confidential medical information to an individual or entity. It contains the patient's name, date of birth, and a description of the medical information to be released. The form also includes the patient's authorization for the release of the information, along with a signature, date, and any other required information.
How to fill out medical records release form?
1. Begin by filling in the patient’s information. This should include their full name, date of birth, and address.
2. Specify the type of medical records you are requesting. This should include the dates of service, type of records, and any other pertinent information.
3. Include the name and address of the person, doctor, or facility that you are requesting the records from.
4. Specify the purpose of the request and the intended recipient of the records.
5. Sign and date the form.
6. Include any additional information or instructions for the doctor or facility.
7. Submit the form to the doctor or facility in person, by mail, or by fax.
What is the purpose of medical records release form?
A medical records release form is used to authorize the release of patient health information to a third party, such as a doctor, hospital, insurance company, or other health care provider. It is important for protecting the privacy of a patient's medical information.
What information must be reported on medical records release form?
A medical records release form typically requires the following information:
- Patient name
- Patient birthdate
- Patient address
- Patient phone number
- Name and address of the recipient of the records
- Purpose for the records release
- Dates and type of records requested
- Patient signature and date of signature
- Witness signature (if required)
Who is required to file medical records release form?
Individuals, healthcare providers, and organizations may be required to file a medical records release form. Patients are typically required to sign a release form to authorize the release of their medical records to other healthcare providers or third parties. Healthcare providers and organizations, such as hospitals or clinics, may also need to file a medical records release form when sharing patients' health information with other healthcare professionals or when providing medical records to patients themselves. Additionally, medical insurance companies may request medical records release forms to access medical information relevant to the evaluation of insurance claims.
What is the penalty for the late filing of medical records release form?
The penalty for the late filing of a medical records release form can vary depending on the specific regulations and legal requirements in place within a particular jurisdiction. Generally, the consequences for late filing may include:
1. Delayed access to medical records: If the medical records release form is not filed on time, it may cause a delay in accessing the requested medical records, which could result in inconvenience for the requesting party.
2. Legal or administrative consequences: In some cases, there may be legal or administrative repercussions for the party responsible for filing the form late. This could include fines, penalties, or potential legal liability if the delay causes harm or violates any laws or regulations.
3. Possible loss of rights or benefits: Late filing may result in the loss of certain rights or benefits associated with accessing or using the medical records. This could impact insurance coverage, eligibility for certain programs or services, or the ability to pursue legal actions related to the medical records.
It is important to consult the specific regulations and policies applicable to your jurisdiction or healthcare system to determine the exact penalties for late filing of medical records release forms.
How can I edit medical records release form from Google Drive?
pdfFiller and Google Docs can be used together to make your documents easier to work with and to make fillable forms right in your Google Drive. The integration will let you make, change, and sign documents, like hipaa medical records release form, without leaving Google Drive. Add pdfFiller's features to Google Drive, and you'll be able to do more with your paperwork on any internet-connected device.
How can I send release of medical records form to be eSigned by others?
laser spine institute tampa medical records is ready when you're ready to send it out. With pdfFiller, you can send it out securely and get signatures in just a few clicks. PDFs can be sent to you by email, text message, fax, USPS mail, or notarized on your account. You can do this right from your account. Become a member right now and try it out for yourself!
Can I edit medical information form on an iOS device?
You can. Using the pdfFiller iOS app, you can edit, distribute, and sign medical form record. Install it in seconds at the Apple Store. The app is free, but you must register to buy a subscription or start a free trial.
Fill out your medical records release form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Release Of Medical Records Form is not the form you're looking for?Search for another form here.
Keywords relevant to laser spine institute medical records form
Related to physician information form


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
